Why in news?
A multi‑institutional study published in 2025 found that about 10 percent of adults with acute lymphoblastic leukaemia carry mutations in the TP53 gene. Patients with these mutations had markedly worse survival outcomes, highlighting the need for tailored therapies. The study’s findings have been widely discussed in 2026, bringing renewed attention to ALL and its management.
Background
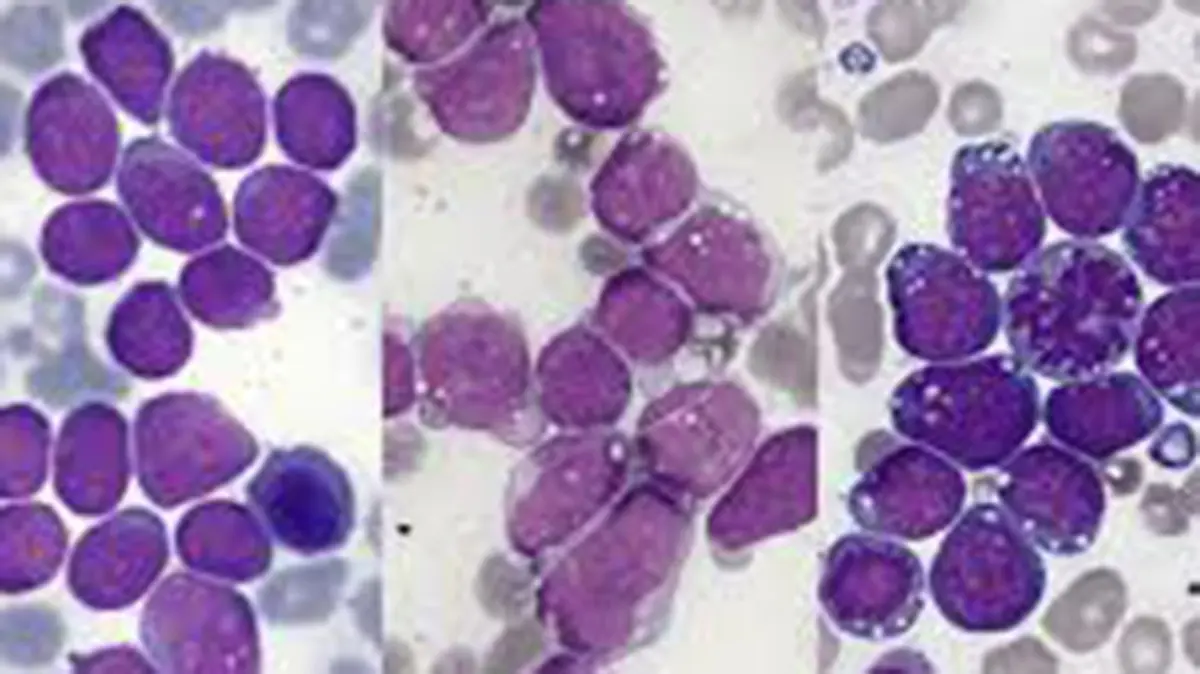
Acute lymphoblastic leukaemia (ALL) is a fast‑growing cancer of the blood and bone marrow. It affects the white blood cells, particularly immature lymphocytes, and can spread quickly if untreated. ALL is the most common type of childhood cancer but also occurs in adults. Common symptoms include bleeding gums, bone pain, fever, frequent infections and unexplained bruising.
Types and risk factors
- B‑cell ALL: The most common form, starting in immature B lymphocytes. It accounts for about 85 percent of childhood cases and roughly 75 percent of adult cases.
- T‑cell ALL: Begins in immature T cells and is less common. Some rare cases involve natural killer (NK) cells.
- Risk factors: Children under 15 and adults over 50 face higher risk. Genetic disorders such as Down syndrome, Fanconi anaemia and exposure to radiation or certain carcinogens increase susceptibility.
Key findings from the 2024–25 study
Researchers analysed 830 adult ALL patients treated between 2010 and 2024. They discovered that about one in ten patients harboured TP53 mutations. These mutations were predominantly missense changes in the DNA‑binding domain and often co‑occurred with hypodiploidy in B‑cell ALL or with NOTCH1/FBXW7 mutations in T‑cell ALL. Patients with TP53‑mutant ALL experienced median overall survival of about 1.9 years in B‑ALL and 1.6 years in T‑ALL, compared with 5 years and 9.5 years respectively for those without the mutation. The study concluded that TP53‑mutant ALL is a distinct, chemo‑resistant entity requiring targeted treatment strategies.
Treatment and outlook
Standard therapy for ALL involves intensive chemotherapy to achieve remission, followed by consolidation and maintenance therapy. Targeted drugs, such as tyrosine kinase inhibitors for Philadelphia chromosome–positive ALL, and immunotherapies like CAR T‑cell therapy have improved outcomes. For high‑risk or relapsed disease, hematopoietic stem cell transplantation may be recommended. The prognosis for children is generally favourable, with cure rates exceeding 80 percent; outcomes are poorer in adults and particularly poor for patients with TP53 mutations.
Conclusion
Understanding the molecular drivers of acute lymphoblastic leukaemia is essential for improving survival. The discovery that TP53 mutations define a high‑risk subgroup underscores the need for routine genetic testing and the development of personalised therapies. Ongoing research into targeted drugs and immunotherapies offers hope for better outcomes in the future.
Source: The Hindu

