Why in news?
Guillain–Barré syndrome has featured in recent health discussions because of isolated cases reported after viral infections. Understanding this rare neurological disorder helps differentiate it from more common conditions and underscores the importance of early medical care.
Background
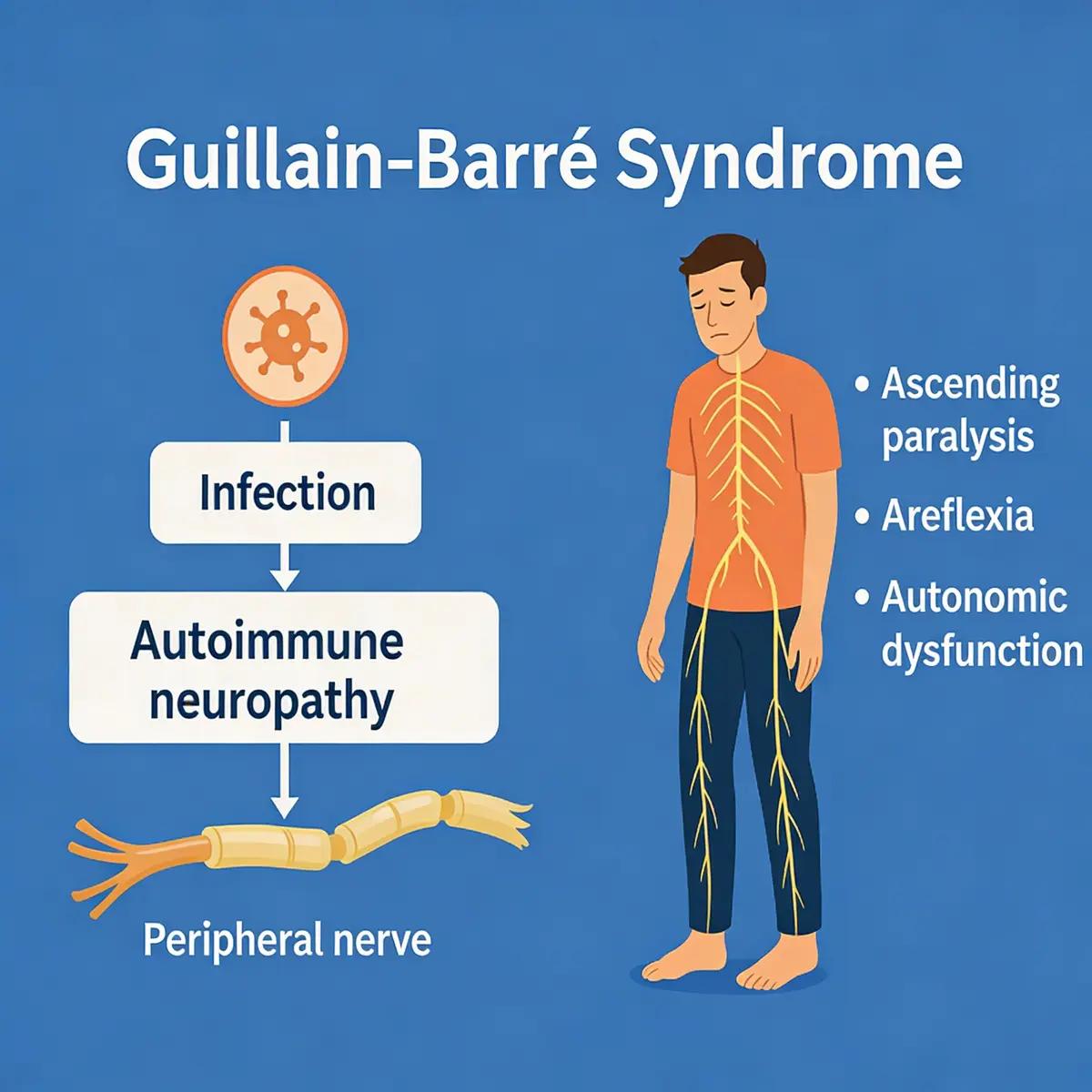
Guillain–Barré syndrome is a rare autoimmune disorder in which the body’s immune system attacks the peripheral nerves. It can occur at any age but is most common in adults between 30 and 50 years old and affects men slightly more than women. In most cases the syndrome develops one to six weeks after a respiratory or gastrointestinal infection. Bacteria such as Campylobacter jejuni and viruses such as influenza, cytomegalovirus, Epstein–Barr and Zika are known triggers. Very rarely, surgery or vaccination may precede the syndrome, but the risk is extremely low compared with the benefits of vaccination.
Symptoms
- Initial signs: Weakness or tingling sensations begin in the feet and legs and may spread to the arms and face. People often describe difficulty walking or climbing stairs and may feel a “pins and needles” sensation.
- Progression: Symptoms can worsen over hours or days. Muscle weakness may advance to paralysis of the legs, arms or facial muscles. About one third of patients experience chest muscle weakness, making breathing difficult.
- Other features: Deep muscle pain, difficulty speaking or swallowing, vision problems, unstable blood pressure and irregular heart rhythms may occur. In severe cases, patients require mechanical ventilation.
- Prognosis: Most people reach maximum weakness within three weeks of onset. With proper treatment, the majority recover fully, although some experience lingering fatigue or weakness. A small number of patients can die from complications such as respiratory failure or blood infection.
Diagnosis and treatment
- Diagnosis: Doctors diagnose GBS based on medical history and neurological examination. Reduced or absent deep‑tendon reflexes are typical. Nerve conduction studies and electromyography can support the diagnosis. A lumbar puncture may show elevated cerebrospinal fluid protein.
- Supportive care: Because GBS can progress rapidly, patients should be admitted to a hospital for close monitoring of breathing, heart rhythm and blood pressure. Some require ventilatory support.
- Immunotherapy: There is no cure, but plasma exchange (plasmapheresis) and intravenous immunoglobulin (IVIG) can reduce severity and shorten recovery if started within 7–14 days of symptom onset.
- Rehabilitation: After the acute phase, physical therapy helps restore strength and mobility. Supportive counselling aids recovery from the psychological impact of sudden paralysis.
Incidence and outlook
- GBS is rare; approximately 100,000 people worldwide develop the syndrome each year, corresponding to about one in 78,000 individuals.
- Both children and adults can be affected, but middle‑aged adults are most frequently diagnosed. Men are slightly more susceptible than women.
- Most patients recover completely, especially when treatment begins early. Ongoing research seeks to understand why the immune system malfunctions in GBS and to develop targeted therapies.
Sources: NDTV