Why in news?
Former Afghanistan fast bowler Shapoor Zadran died at age 38. The Afghanistan Cricket Board announced his death on 7 July 2026, and he had reportedly been diagnosed with HLH. The case brought this rare immune disorder into public attention.
Background
Hemophagocytic lymphohistiocytosis is usually shortened to HLH, and it is a rare and life-threatening hyperinflammatory syndrome. The immune system becomes severely overactive and cannot switch itself off.
Normally, cytotoxic T cells and natural killer cells remove infected cells. In HLH, this control system does not work properly, and activated immune cells continue releasing inflammatory proteins called cytokines.
This uncontrolled reaction is called a cytokine storm and can damage the liver, spleen, bone marrow and brain. Severe cases may progress to failure of several organs.
What does the name mean?
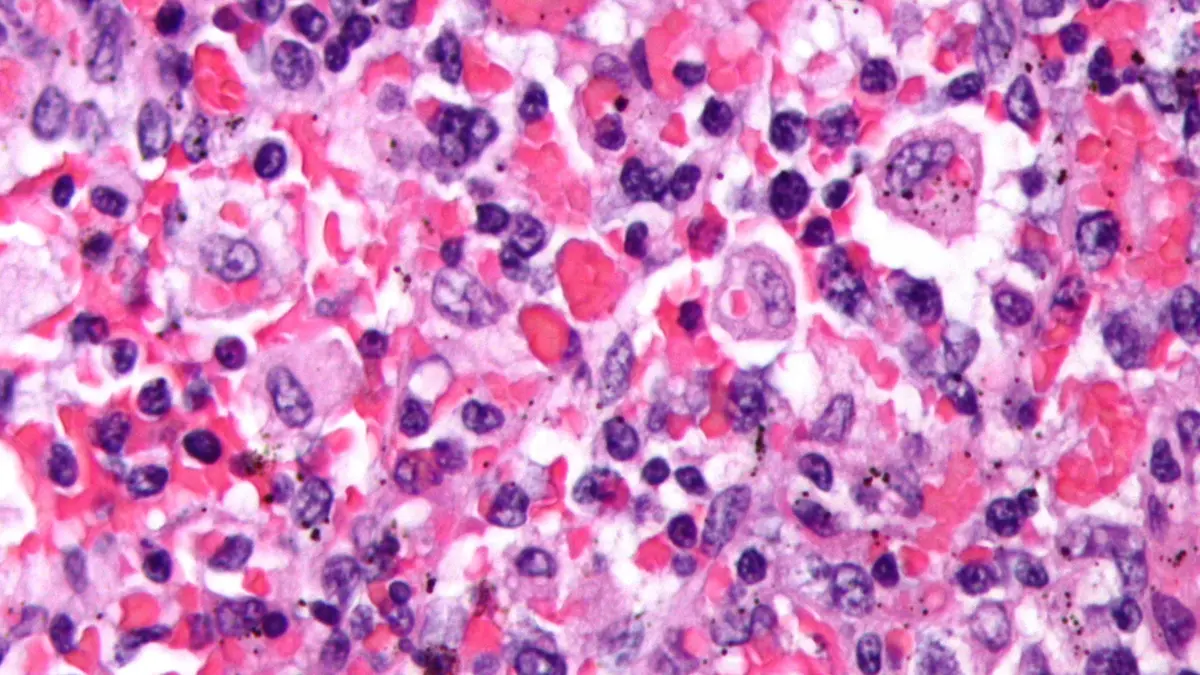
- Hemophagocytic refers to immune cells engulfing blood cells; Lympho refers to lymphocytes, which are white blood cells.
- Histiocytosis refers to increased activity of tissue macrophages or histiocytes.
Hemophagocytosis may be visible in bone marrow, but it can be absent during early disease. Its absence alone cannot rule out HLH.
Two broad forms
- Primary or familial HLH: Inherited gene changes impair immune-cell regulation. It often appears in infancy or childhood. Some patients first develop symptoms as adults.
- Secondary or acquired HLH: Another illness triggers the immune overreaction. This form is more common among adults.
Familial HLH is commonly inherited in an autosomal recessive pattern. If both parents carry the same variant, each pregnancy has three possibilities. The child has a 25% chance of disease and a 50% carrier chance. There is also a 25% chance of inheriting neither altered copy.
Common triggers of secondary HLH
- Viruses can trigger HLH, especially Epstein–Barr virus.
- Bacterial, fungal and parasitic infections can also trigger it.
- Blood cancers can trigger HLH, including lymphoma and leukaemia.
- Autoimmune and autoinflammatory diseases are other possible triggers.
- Some medicines and states of immune suppression can also trigger HLH.
HLH linked with rheumatic disease is often called macrophage activation syndrome, and the underlying mechanism overlaps with secondary HLH.
Symptoms and warning signs
- A persistent high fever is common, while the liver and spleen may enlarge.
- Blood cell counts may fall, causing severe tiredness, pallor and easy bleeding.
- Patients may develop jaundice, rashes or swollen lymph nodes; some develop confusion, seizures or other neurological symptoms.
The symptoms resemble severe infection or sepsis, and this similarity can delay diagnosis. Doctors therefore combine clinical signs with several laboratory results.
How is HLH diagnosed?
A known HLH-linked genetic mutation can establish the diagnosis, and otherwise, doctors commonly use eight published criteria. A patient generally must meet at least five.
These criteria include fever, enlarged spleen and low blood-cell counts, and they also include high triglycerides or low fibrinogen. Other markers include very high ferritin and raised soluble interleukin-2 receptor.
Reduced natural-killer-cell activity is another criterion, and evidence of hemophagocytosis may also support diagnosis. No single blood test is enough in every case.
Treatment
HLH is a medical emergency, and treatment must suppress the dangerous inflammation. Doctors must also identify and treat the trigger.
Dexamethasone and etoposide are established medicines in many protocols, and other immune-targeting medicines may be used in selected cases. Infections or cancers need their own specific treatment.
Primary HLH often requires a donor stem-cell transplant after initial control, and transplantation replaces the defective immune system. It may also help recurrent or treatment-resistant disease.
Conclusion
HLH turns the body’s defence system into a source of organ damage. Early recognition is difficult but crucial, and prompt specialist treatment can greatly improve the chance of survival.